Depth-Perception Device with Direct Feedback for
Laparoscopic Skills Training
Through ethnographic efforts in the Pittsburgh area, my group and I identified an unmet need in the Laparoscopic Training field:
Low Tech Training
This type of training includes experiential methods, such as practicing moving a pea from point A to point B. While these methods prove easily implemented and accessible, none target a single, specific skill or provide the user with any feedback.
The specific skill that we chose to target was depth perception--interpreting a 2D screen as a 3D surgical field--as this is the first and most difficult task students must master.

High Tech Training
High tech training involves virtual reality simulation, where there are a multitude of specific skill modules as well as realistic surgeries. This technology provides immediate metric feedback. However, these devices are extremely expensive, and if available in a clinic, only one student can use it at a time.
The specific skill that we chose to target was depth perception--interpreting a 2D screen as a 3D surgical field--as this is the first and most difficult task students must master.
Standardized Assessment
While students can utilize any combination of low and high tech options, they must all pass a high, risk Fundamentals of Laparoscopic Surgery (FLS) assessment in order to take their Board Examinations. FLS includes 5 basic tasks like a peg transfer below, where number of errors and time are monitored.
The specific skill that we chose to target was depth perception--interpreting a 2D screen as a 3D surgical field--as this is the first and most difficult task students must master.
Proposed Solution
By incorporating some advantageous, basic elements of high-tech
training, such as direct feedback, into a more accessible and/or
applicable low-tech application, this device gap can be bridged to
provide students with a method for improving their initial learning curve
and skill retention.
The specific skill that we chose to target was depth perception--interpreting a 2D screen as a 3D surgical field--as this is the first and most difficult task students must master.



6 user needs were identified through pretotyping efforts, addressing dimensional compatibility between our device and standard FLS training boxes, randomization, training of multiple depths, durability and portability of product, and accessibility in the form of direct feedback to the user without an educator present.
Personal Contributions to Senior Design Team
1.
Led group organization efforts via Gantt Chart methods and acted as point of contact between the group & clinicians/mentors and other team leads.
2.
Designed the device Depth-Perception Device and all removable components in Solidworks; subsequently laser cut each component in hardboard material
3.
Contributed to Arduino code development and NeoPixel LED, buzzer circuitry, and LCD screen development
4.
Contributed to final device fabrication and installation of hand-made peg-units of silicone tubing and conductive copper foil.
5.
Led all Pitt IRB contact efforts for validation testing execution of the final device, receiving approval after clarifications.
6.
Contributed to 3-minute Video creation as a supporting validation effort following the inability to execute planned validations due to the COVID-19 pandemic.
7.
Contributed to poster creation and presentation at Pitt's Fall 2019 Design Expo.
Prototype Development
The image below follows the progression of our prototypes throughout the fall semester which, at their core, are boards with pegs of various depths that users must grasp went prompted within a specified amount of time in order to sound a buzzer.
The left most is our pretotype, used to identify crucial basic functions of our solution and their facets that clinicians liked best, such as peg height, visual guidance via LED firing, and basic feedback in the form of buzzing upon proper grasping.
The middle image is our Prototype #1, including one peg/LED unit and a "gift box"-like board design. This prototype helped us evaluate the optimal peg flexibility, the pegs’ spacing throughout the device, the comfortability of the device, and its ease of implementation in standard FLS boxes.

Pretotype Prototype 1 Prototype 2
Prototype 2
Pictured in more detail below, the device also includes a supplemental phone holder. The following components are included:
-
Arranged LED lights (red = left hand-, blue = right hand-instrument grasping) for dominant and non-dominant hand training
-
Arduino generating random LED light firing for 8 second durations, lending for session-to-session variation and optimal times for beginner-learners to achieve
-
Easy button to power the entire device via 9-V battery
-
Wiring along flexible silicone tubes that, when grasped properly, complete a circuit and buzz, providing auditory feedback
-
Adjustable phone holder for session recording/review


GOALS ACHIEVED FOR
PROTOTYPE 3
-
Make pegs lower profile, utilizing conductive copper foil instead of bulky wiring
-
Optimize peg-unit spatial organization
-
Improve cord management within the board using tools like ribbon wire and male/female headers
-
Incorporate some form of basic quantitative feedback via Arduino coding and LCD screen display/drawer
-
Create battery holder drawer that is easily accessible to the user without having to "open" the device board
-
Improved Phone Holder stand, propping phone up at multiple angles with silicone edges for friction
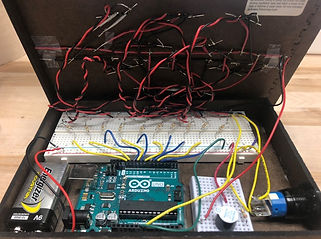
FINAL PROTOTYPE 3

The Depth-Perception Training device with A. the device turned off, B. the removable battery holder panel, C. the device turned on with the LCD display pulled out, and D. circuitry elements within the device, including NeoPixel LED light and buzzer wiring, LCD Display, 9V battery/holder, power button, circuit board, and Arduino.
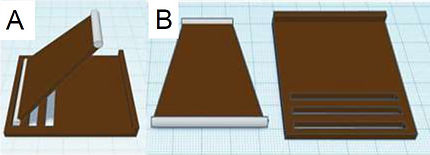
Digital illustration of supplemental phone holder A. in use and B. with the trapezoid stand (featuring silicone-edges) and base (with multiple slits for various phone angling) components separated
INSTRUCTIONAL VIDEO

Verification and Validation Efforts
VERIFICATION
-
Product dimensions to fit within a standard FLS training box and be compatible with laparoscopic instruments
-
Functional requirements for LED instructive cues, LCD screen quantitative feedback, and buzzing auditory feedback
-
Product Weight for portability and ease of use
-
Product Cyclic Stresses to last 2 months (15 uses/week, 30 grasps/use)
RESULTS
-
Dimensional testing confirms the entire device can fit within a standard FLS trainer box and be visualized within the projected 2D screen
-
Functional testing confirmed randomization of LED firing and proper display of training scores on the LCD screen
-
The weight of the device was < 5 pounds; phone holder weight was unable to be performed due to the COVID-19 pandemic.
-
No visual lesions or breakage were observed after cyclic stressed were applied
VALIDATION
-
Beginner-learner and educator/clinician opinion of the device's usability and applicability in advancing depth-perception skills after viewing a 3-minute instructional video
Ex beginner-learner question (1-5, where 5 means strongly agree):
-
I think it would be easy to transport, install, turn on, and overall interact with the device by myself.
Ex educator question (1-5, where 5 means strongly agree)
-
I would feel comfortable integrating this device into already existing training methods.
RESULTS
-
Both beginner-learners and educators/clinicians showed over an average of 70% positive opinions regarding the device's efficacy (3.5/5)
-
The highest average score (4.625) for beginner-learners was in regards to the device's ability to provide immediate feedback to help the user learn correctly
-
Educator average scores were all ~4.4/5, indicating their confidence in integrating this device into standard training
Note: A validation comparability study was approved by Pitt IRB as Exempt Educational. This study included students training with already available low-tech modules with the possible addition of our device--before and after FLS Peg-Transfer test scores would be recorded to evaluate any statistical different in user performance with or without our device. However, due to the COVID-19 pandemic, this study was unable to be executed but may be completed at a later date.
In all, we were able to:
-
Identify an unmet need
-
Describe necessary design specifications
-
Identify and mitigate risk via risk analyses methods like IHA, FTA, and FMEA
-
Prototype and re-iterate based on these analyses
-
Test a final product through verification and validation efforts
Through this experience I learned many fabrication techniques as well as the fundamentals of product design in alignment with 21 CFR 820.30 Design Controls.
We hope to give our device to the clinicians and educators that we collaborated with, allowing for them to fully integrate the device into their daily trainings!
SPECIAL THANKS!
Thank you so much to Dr. Donnellan, Dr. Newcomb, Dr. Hamad, Dr. Samosky and our professor Dr. Gartner for guiding us in this project.